Case Report
Corticotomy facilitated correction of skeletal class II malocclusion

Arif Yezdani A*
Department of Orthodontics and Dentofacial Orthopedics, Professor and Director, Bharath University, Sree Balaji Dental College and Hospital, Narayanapuram, Pallikaranai, Chennai-600100, Tamilnadu, India*Address for Correspondence: Arif Yezdani A, Department of Orthodontics and Dentofacial Orthopedics, Professor and Director, Bharath University, Sree Balaji Dental College and Hospital, Narayanapuram, Pallikaranai, Chennai-600100, Tamilnadu, India, Email: [email protected]
Dates: Submitted: 10 October 2017; Approved: 25 October 2017; Published: 26 October 2017
How to cite this article: Yezdani AA. Corticotomy facilitated correction of skeletal class II malocclusion. J Oral Health Craniofac Sci. 2017; 2: 096-103. DOI: 10.29328/journal.johcs.1001018
Copyright License: © 2017 Yezdani AA. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Supernumerary premolars; Decortication; Bone graft; Rapid orthodontics
Abstract
Introduction
Adult or late adolescent patients requiring orthodontic correction of malocclusion desire short treatment periods due to social and psychological reasons which is feasibly possible only in conjunction with surgical procedures [1,2]. Orthopedist Harold Frost termed the cascade of physiologic healing events following surgical wounding of cortical bone the Regional Acceleratory Phenomenon (RAP) [3,4]. This phenomena is taken advantage of in bringing about rapid orthodontic tooth movement which together with periodontal augmentation with bone graft increases the alveolar bone housing as also corrects alveolar bone dehiscences and fenestrations [5]. The bone graft provides additional bone support, resulting in less tendency for relapse [6]. It also improves the posture of the lip in certain conditions. Animal experiments too have demonstrated an increase in apposition and resorption of alveolar spongiosa adjacent to corticotomy cuts [7]. Hence, circumscribed corticotomy cuts and augmentation with bone graft was found to increase the rate of orthodontic tooth movement and shorten the period of orthodontic treatment in the case reported.
Case Report
A male patient aged 25 years presented with forward placement of maxillary anteriors and crowded mandibular anteriors with bilateral supernumerary premolar teeth in maxillary dental arch.
Extra-oral assessment
The patient had a mesoprosopic face, convex profile, posterior divergence, incompetent lips, clinical low mandibular plane angle and excessive maxillary incisor display on smiling, with no signs of temporomandibular joint dysfunction (Figure 1a-c).
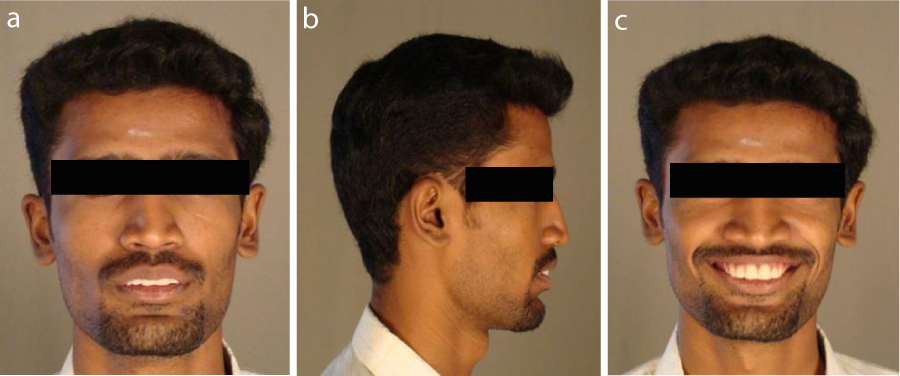
Figure 1: a). Pre treatment extraoral – Frontal; b). Pre treatment extraoral – Profile; c). Pre treatment extraoral – Smiling.
Intra-oral assessment
Oral hygiene was satisfactory. Maxillary arch was U-shaped, asymmetrical with a supernumerary premolar present bilaterally in the premolar region, impacted UL5 and proclined maxillary incisors. Mandibular arch was U-shaped, asymmetrical with proclined, rotated and imbricated mandibular incisors.
In occlusion, increased overjet and deep bite was observed. The maxillary dental midline was shifted to the left by 1mm,and on left side the molar relation was class II and on the right it was class I while the canine relation was end-on bilaterally with UL5 and UL6 in mild palatal cross-bite (Figure 1d-h).

Figure 1D-H: d). Pre treatment intraoral - Frontal e). Pre treatment intraoral – Right; f). Pre treatment intraoral – Left; g). Pre treatment intraoral - Upper occlusal; h). Pre treatment intraoral - Lower occlusal.
Radiographic assessment
The panoramic radiograph confirmed the presence of all permanent teeth, and normal alveolar bone levels except around impacted UL5, with impacted LR7 and LL8 with partially erupted UR8 and UL8 (Figure 2).

Figure 2: Pre treatment panoramic radiograph.
Cephalometric analysis revealed a skeletal Class II pattern with an orthognathic maxilla and retrognathic mandible, with a low mandibular plane angle, severely proclined maxillary incisors and moderately proclined mandibular incisors (Figure 3).

Figure 3: Pre treatment lateral cephalometric radiograph.
Aims and objectives
1. Improve oral hygiene.
2. Improve facial profile and achieve lip competence.
3. Correction of protruded maxillary and mandibular teeth.
4. Correction of imbricated and rotated mandibular teeth.
5. Correction of end-on canine relationships.
The patient opted for the corticotomy procedure as he preferred the orthodontic treatment to be completed within a short period of time. Extraction of supernumerary in the maxillary right and left premolar region and impacted UL5 was done. Roth’s prescription Pre Adjusted Edgewise Appliance Therapy (0.022x0.028-inch slot), (3M Unitek, Monrovia, CA, USA) with upper and lower 0.014-inch nickel titanium archwires along with transpalatal anchorage was strapped a week prior to the surgical procedure.
The patient underwent decortication of the alveolar bone and grafting with Grabio Glascera bone graft. (DORTHOMTM MEDI DENTS PVT. LTD., Coimbatore, Tamil Nadu, India). Grabio Glascera (GG) are bioactive, ceramic, composite, porous granules made up of:- 50% Bioactive Glass (BG) and 50% Hydroxyapatite (HA) mixture available in a particle size of 0.15 - 0.50 mm.
Orthodontic adjustments were made at 2 week intervals.
Surgical procedure
Under local anesthesia, labial and lingual sulcular incisions were made and full thickness mucoperiosteal flaps were elevated without disturbing the neurovascular bundles and the genioglossus attachment. A long shank surgical fissure bur was used to make the corticotomy cuts barely into the medullary bone on labial and lingual aspects of maxillary and mandibular anterior teeth alongside the roots with a scalloped cut slightly above the apices of the teeth. One to two mL of platelet rich plasma from the patient’s blood was mixed with GG granules and placed over the decorticated area. The flaps were then returned to their original position and sutured with one interrupted loop 3/0 suture, interproximally (Figure 4a-b, Figure 5a-b, Figure 6a-c).
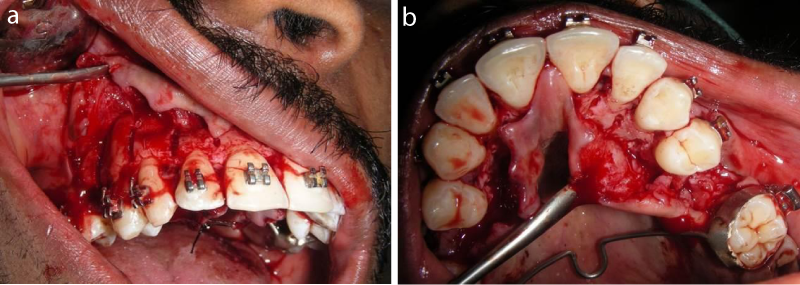
Figure 4: a). Circumscibing corticotomy cuts-maxillary labial view; b). Circumscibing corticotomy cuts - maxillary palatal view.
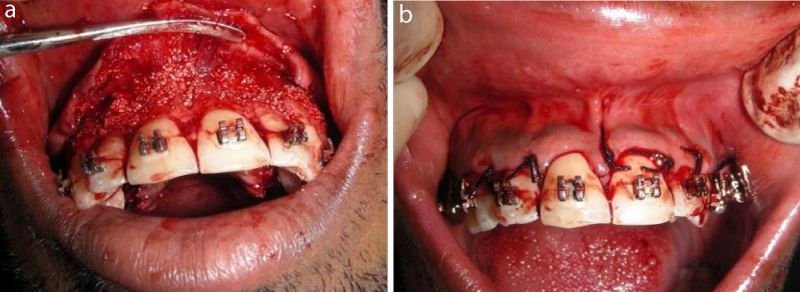
Figure 5: a). Alveolar augmentation with Grabio Glascera bone graft - maxillary anterior view; b). Suturing.
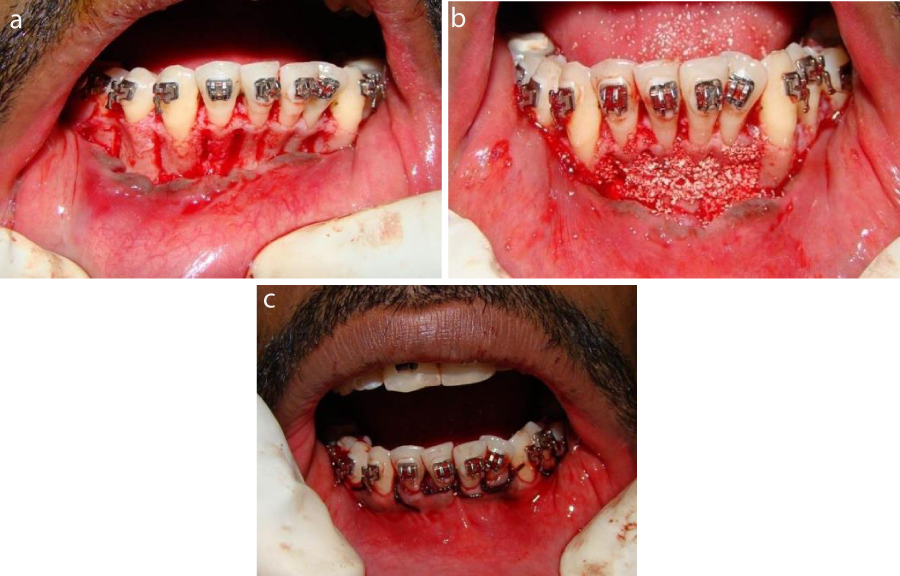
Figure 6: a) Circumscibing corticotomy cuts - mandibular anterior view; b). Alveolar augmentation with Grabio Glascera graft - mandibular anterior view; c). Suturing.
Amoxycillin 500mg t.id./week and anti-inflammatory drugs t.i.d/week were prescribed. An antiseptic mouthwash was advised. Two weeks later the sutures were removed and non-steroidal anti-inflammatory drugs were asked to be discontinued as they would interfere with orthodontic tooth movement.
Orthodontic procedure
The orthodontic treatment was commenced immediately after suture removal. Initial aligning and levelling was done with upper and lower 0.014-inch nickel titanium archwires, upgraded to 0.016-inch nickel titanium archwires. Extraction space closure for the maxillary dental arch was done with 9mm nickel titanium closed coil springs attached to crimpable hooks on 0.017x0.025-inch stainless steel archwires. Detailing and finishing was done with upper and lower 0.019x0.025-inch stainless steel archwires (Figure 7a-b).
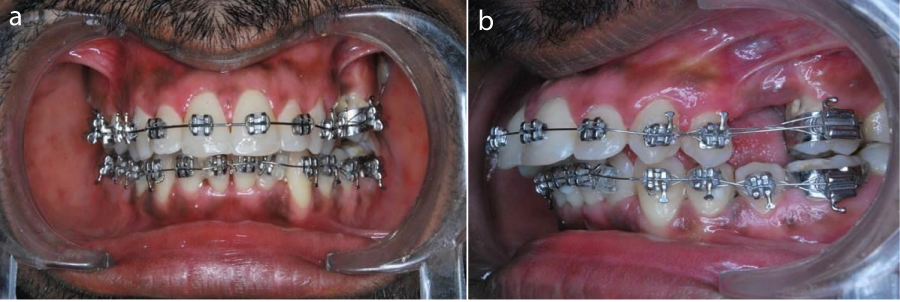
Figure 7: a). Orthodontic treatment - Frontal view; b). Orthodontic treatment - Left view.
Discussion
The patient showed remarkable improvement in his soft tissue profile and smile esthetics (Figure 8a-c). The bi-maxillary dentoalveolar protrusion, increased overjet, rotated and imbricated mandibular incisors was corrected in nine months (Figure 9a-e, Figures 10,11). The rapid correction of the malocclusion was most probably attributed to the RAP phenomena triggered by the corticotomy procedure which caused an increase in the osteoclastic activity of the bone. The resultant osteopenia was responsible for the rapid tooth movement that was observed. Corticotomy with bone augmentation increased the volume of the bone and maximized the metabolic response during orthodontic treatment in concert with what has been reported in literature [8]. Care was also taken to thin the bone on the distal aspect of the canine roots during the corticotomy procedure. Full thickness mucoperiosteal flaps have been used in the case reported. However, conservative flapless corticotomy techniques have also been recently proposed to mitigate the invasiveness of the full mucoperiosteal flaps [9]. No loss of tooth vitality, discoloration or pain was observed in tune with what has been reported in literature [10-12]. In conventional orthodontics, due to prolonged treatment duration or inadvertent application of heavy forces root resorption is observed [13]. In the case reported no root resorption was observed because of bone matrix transportation and reduced density of the bone due to osteopenia created by the corticotomy procedure. The patient was seen every 2 weeks, throughout the phases of aligning, levelling, space closure, finishing and detailing to take advantage of RAP.

Figure 8: a). Post treatment extraoral – Frontal; b). Post treatment extraoral - Profile; c). Post treatment extraoral – Smiling.
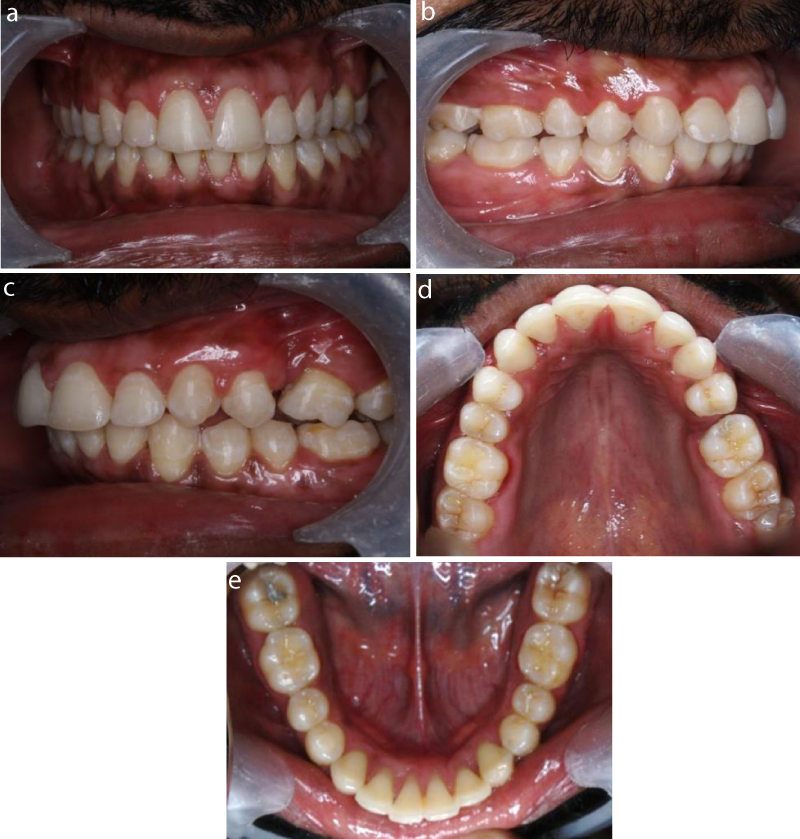
Figure 9: a). Post treatment intraoral – Frontal; b). Post treatment intraoral – Right; c). Post treatment intraoral – Left; d). Post treatment intra-oral - Upper occlusal; e). Post treatment intra-oral - Lower occlusal.

Figure 10: Post treatment panoramic radiograph.

Figure 11: Post treatment lateral cephalometric radiograph.
The periodontal alveolar augmentation with the GG bone graft increased the bone volume thereby reducing the incidence of relapse a thing often observed when orthodontic treatment is done without bone grafting. This procedure is also useful for thinner mandibular cortices which are at increased risk for relapse subsequent to dental de-crowding [14]. Fixed lingual retainers were given for both maxillary and mandibular dental arches. The rapid correction of the malocclusion had been made possible because of the cortiocotomy facilitated procedure, which also reinforces a claim made in literature that results are more stable with minimal risk of complications with faster orthodontic treatment after a corticotomy procedure [15]. Corticotomy facilitated orthodontics greatly contributed to the completion of the correction of the malocclusion in one-third to three-fourth the time required for conventional orthodontics.
Conclusion
The corticotomy facilitated orthodontics speedied up the correction of the malocclusion in just about nine months and the alveolar augmentation with the bone graft provided an increased bone volume to house the dentition. This created a stable and conducive environment to mitigate the occurrence of the tell-tale relapse.
References
- Roblee RD, Bolding SL, Landers JM. Surgically facilitated orthodontic therapy: a new tool for optimal interdisciplinary results. Compend Contin Educ Dent. 2009; 30: 264-275. Ref.: https://goo.gl/8wr1V5
- Dibart S, Sebaoun JD, Surmenian J. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent. 2009; 30: 342-344, 346, 348-350. Ref.: https://goo.gl/dFyffb
- Frost HM. The biology of fracture healing: An overview for clinicians. Part I. Clin Orthop Relat Res. 1989; 248: 283-293. Ref.: https://goo.gl/fEFkAb
- Frost HM. The biology of fracture healing: An overview for clinicians. Part II. Clin Orthop Relat Res 1989; 248: 294-309. Ref.: https://goo.gl/Jc2t8y
- Wilcko MW, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001; 21: 9-19. Ref.: https://goo.gl/5HnJsE
- Wilcko MW, Ferguson DJ, Bouquot JE, Wilcko MT. Rapid Orthodontic De-crowding with Alveolar Augmentation: Case Report. World J Orthod. 2003; 4: 197-205. Ref.: https://goo.gl/JE4Pdt
- Sebaoun JD, Ferguson DJ, Wilcko MT, William WM. Corticotomie alveolaire et traitements orthodontiques rapides. Orthod Fr. 2007; 78: 217-225. Ref.: https://goo.gl/soxzVe
- Wilcko MT, Wilcko WM, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: a synthesis of scientific perspectives. Semin Orthod. 2008; 14: 305-316. Ref.: https://goo.gl/3pFYXz
- Suya H. Corticotomy in orthodontics. In: Hosl E, Baldauf A, editors. Mechanical and biological basics in orthodontic therapy. Heidelberg, Germany: Huthig Buch Verlag: 1991; 207-226.
- Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament. Am J Orthod Dentofacial Orthop. 1998; 114: 372-382. Ref.: https://goo.gl/QwRjG5
- Sukurica Y, Karaman A, Gurel HG, Dolanmaz D. Rapid canine distalization through segmental alveolar distraction osteogenesis. Angle Orthod. 2007; 77: 226-236. Ref.: https://goo.gl/QuLU4C
- Iseri H, Kisnisci R, Bzizi N, Tuz H. Rapid canine retraction and orthodontic treatment with dentoalveolar distraction osteogenesis. Am J Orthod Dentofacial Orthop. 2005; 127: 533-541. Ref.: https://goo.gl/JcAmq7
- Rygh R, Brudvik P. The histological responses of the periodontal ligament to horizontal orthodontic loads.In:Berkovitz BKB,Moxham BJ,Newman HN(eds).The Periodontal ligament in Health and Disease.London:Mosby-Wolfe.1995: 250-254.
- Rothe LE, Bollen RM, Herring SW, Herring SW, Chaison JB, et al. Trabecular and cortical bone as risk factors for orthodontic relapse. Am J Orthod Dentofacial Orthop. 2006; 130: 476-484. Ref.: https://goo.gl/XpLAVZ
- Kole H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol. 1959; 12: 515-529. Ref.: https://goo.gl/eXktzx